The Ground Reality: What's Actually Getting in the Way
To set the stage, attendees were asked about their biggest challenges in managing patient access, beyond the well-known clinician shortage.
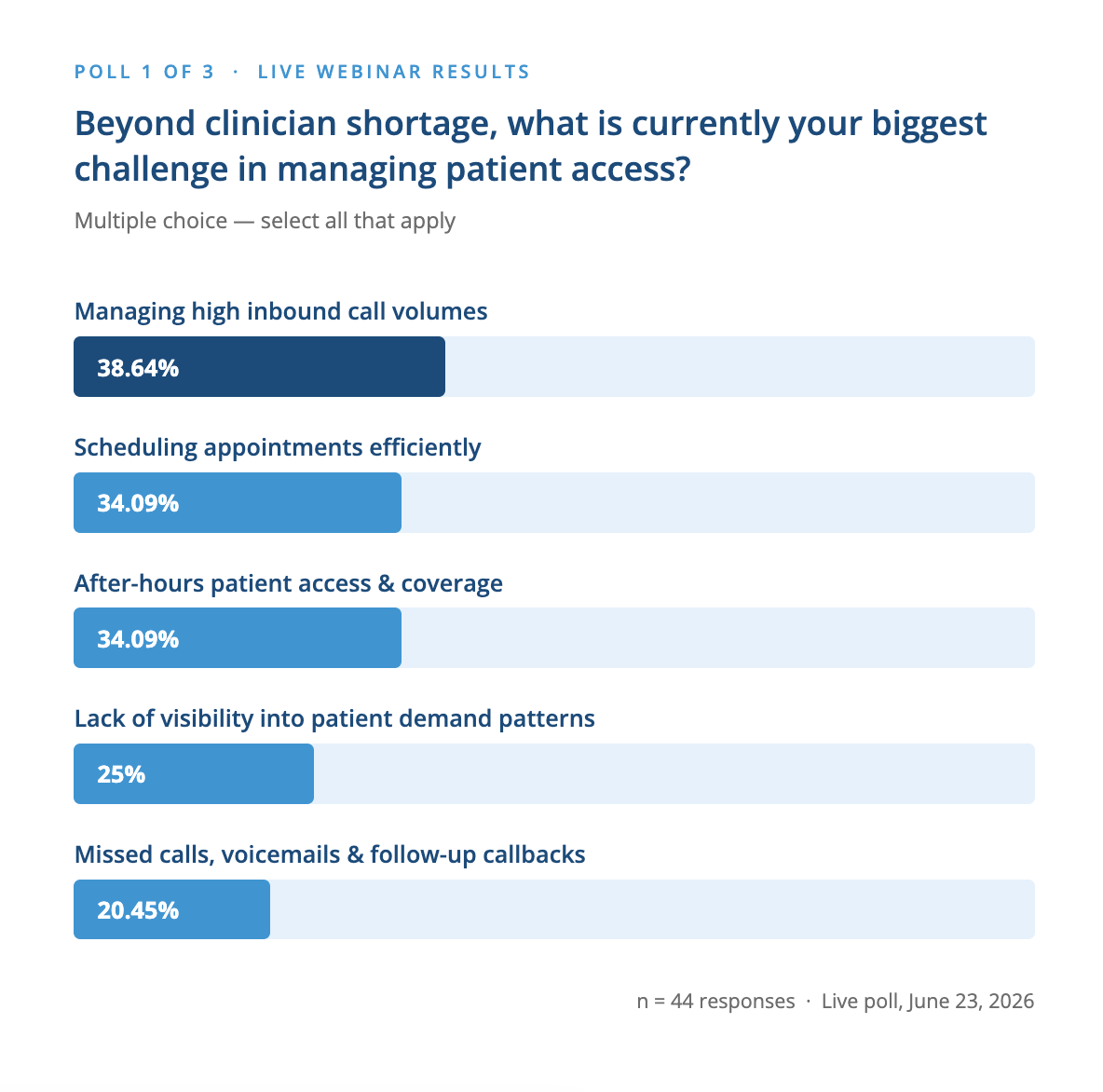
Managing high inbound call volumes topped the list at nearly 39%, followed closely by scheduling efficiency and after-hours coverage. The results confirm what those working in and around primary care already feel: the access problem is a workflow and coordination problem as much as a capacity one. These challenges are deeply interconnected. High call volumes lead to missed calls, which lead to scheduling inefficiencies and patients falling through the cracks.
From the Front Lines: Dr. Dan Pepe on Running a Growing Practice
Dr. Dan Pepe, family physician at London Lambeth Family Medicine Clinic in London, Ontario, has lived this firsthand. Running a comprehensive practice of roughly 2,200 rostered patients alongside his wife Dr. Cassandra Lin-Pepe, he described how operational complexity accumulates quietly over time.
For Dr. Pepe, triage has become one of the central challenges of running a modern practice. Having cycled through six or seven medical secretaries over eight years, he emphasized that front desk staff are arguably a clinic's most important, and most underserved resource. Without the time to properly train staff or build robust triage processes, the wrong patients end up being seen too often while the right ones can't get in when they need to.
The approach that eventually emerged? Routing all calls to voicemail, stack-ranking them by urgency, and working through the queue. It was functional, but it created a different problem. Call volume never really calmed down throughout the day, leaving admin staff stretched from open to close with little uninterrupted time to execute on tasks.
The Solution: IDENTOS + OneChart, Built for Primary Care
This is where Shreyas Suri, CEO and founder of OneChart, entered the picture. OneChart is an AI workflow automation company for healthcare, focused on making clinical operations more structured and manageable.
The collaboration was grounded in a first-principles approach: rather than layering new technology on top of existing processes, the team mapped actual workflows at the practice and identified where AI could reduce friction without compromising clinical judgment.
At its core, the solution replaces an unstructured voicemail process with a structured, AI-powered Voice Intake system that collects the right information, every time, so that when a staff member goes to action a message, they already have what they need to move.
IDENTOS's role in the stack is foundational. The solution is built on IDENTOS's secure access exchange and Federated SSO, integrated with OneChart's AI Voice Agent suite — together providing the clinic's team with a centralized command center to review and action incoming patient conversations in real time.
As IDENTOS has been supporting Ontario and other provincial health systems since 2014, this infrastructure is designed to scale: from a single-location family practice to multi-site OHT deployments.
OneChart's AI Voice Agent suite sits at the front end of this stack, handling the intake conversation itself, collecting structured, verified information and routing it into the command center where the clinical team can act on it.
What the AI Actually Does (and Doesn't Do)
A critical point raised throughout the webinar: the AI voice agent is not replacing clinical triage. It is not making medical decisions. What it does is collect structured, verified information, such as patient name, callback number, prescription renewal requests, reason for visit, so that the human team can triage with far more context than a standard voicemail provides.
All AI workflows follow a human in the loop process, where final actions are verified by a team member before being taken forward.
Two live demonstrations gave attendees a clear look at how this works in practice:
Demo 1: Prescription Renewal The AI agent guided a caller through confirming their name , callback number, medication name and dosage, preferred pharmacy and location, and email address for follow-up — all verified back in real time. At the end, it informed the caller that the clinical team would review the request and determine whether it could be renewed directly or if an appointment would be needed.
Demo 2: Appointment Booking The agent collected details about the patient's presenting symptoms (seasonal allergies, plus secondary back pain), confirmed their preferred contact method, and proactively noted scheduling constraints. For example, Dr. Pepe is in the operating room on Wednesdays and unavailable in the office that day. The conversation was adaptive, picking up on additional context the patient shared organically.
Both demos illustrated a key design principle: the agent's questions adapt in real time, based on what the caller says, which means the messages the clinical team receives are richer and more actionable than a typical voicemail.
Poll 2: What Does the Industry Think?
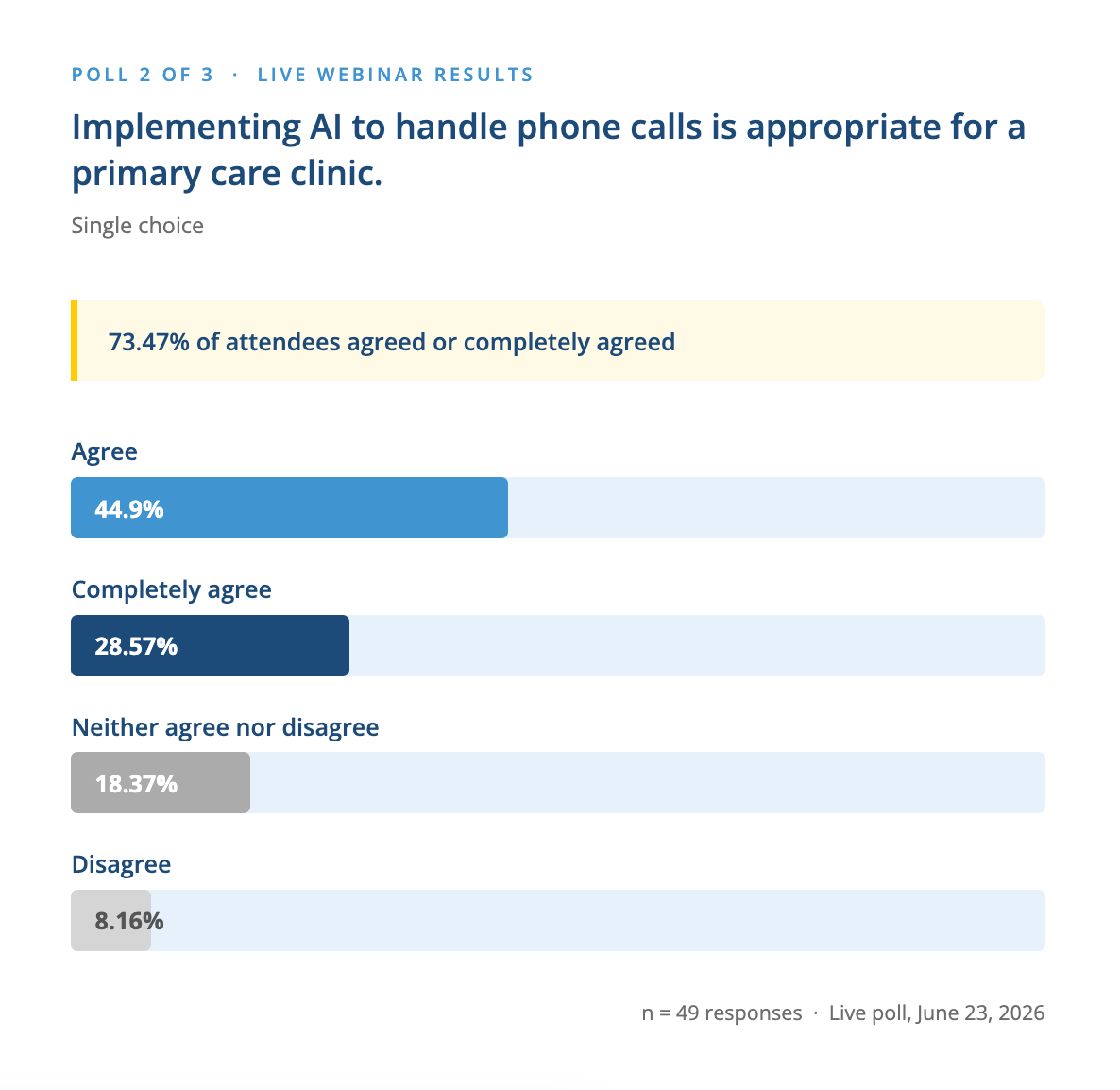
Nearly three quarters of respondents agreed or completely agreed. For those in the disagree or neutral camp, the framing matters: the AI is handling information collection, not clinical assessment. The Medical Office Receptionist's role doesn't disappear, but rather, gets elevated. When a team member calls a patient back, they already know the medication, the pharmacy, the reason for the visit. They can get right to helping, and acting on the information.
Pilot Results: What the Data Showed
OneChart and Dr. Pepe's clinic ran a structured Phase 1 pilot over 22 active clinic days. The results were concrete:
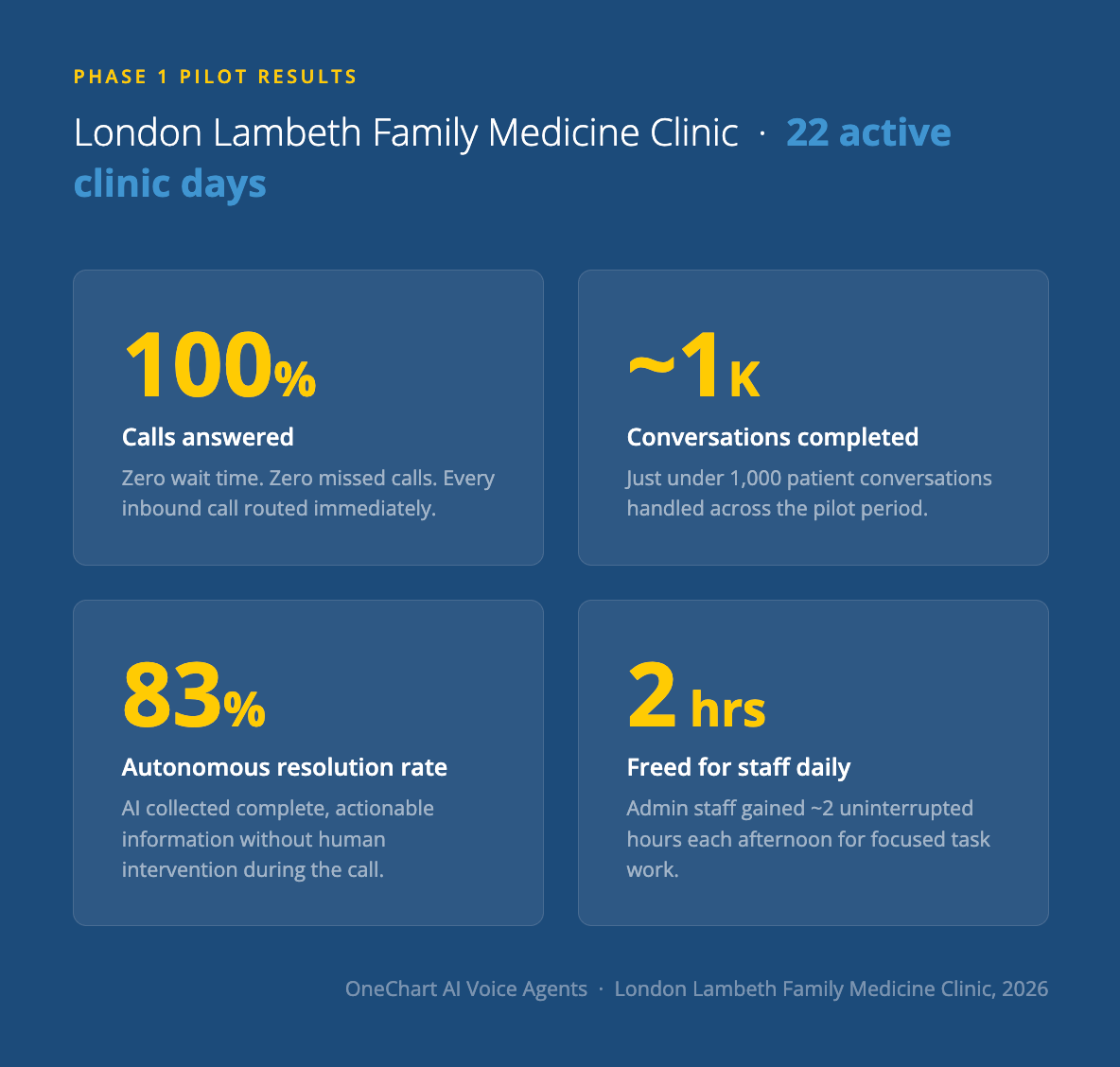
Across the call categories tracked, the highest resolution rates came from appointment requests, reschedules, prescription renewals, and clinical inquiries. The lowest came from highly specific or unclassified requests, an expected finding that OneChart is addressing iteratively as the knowledge base grows.
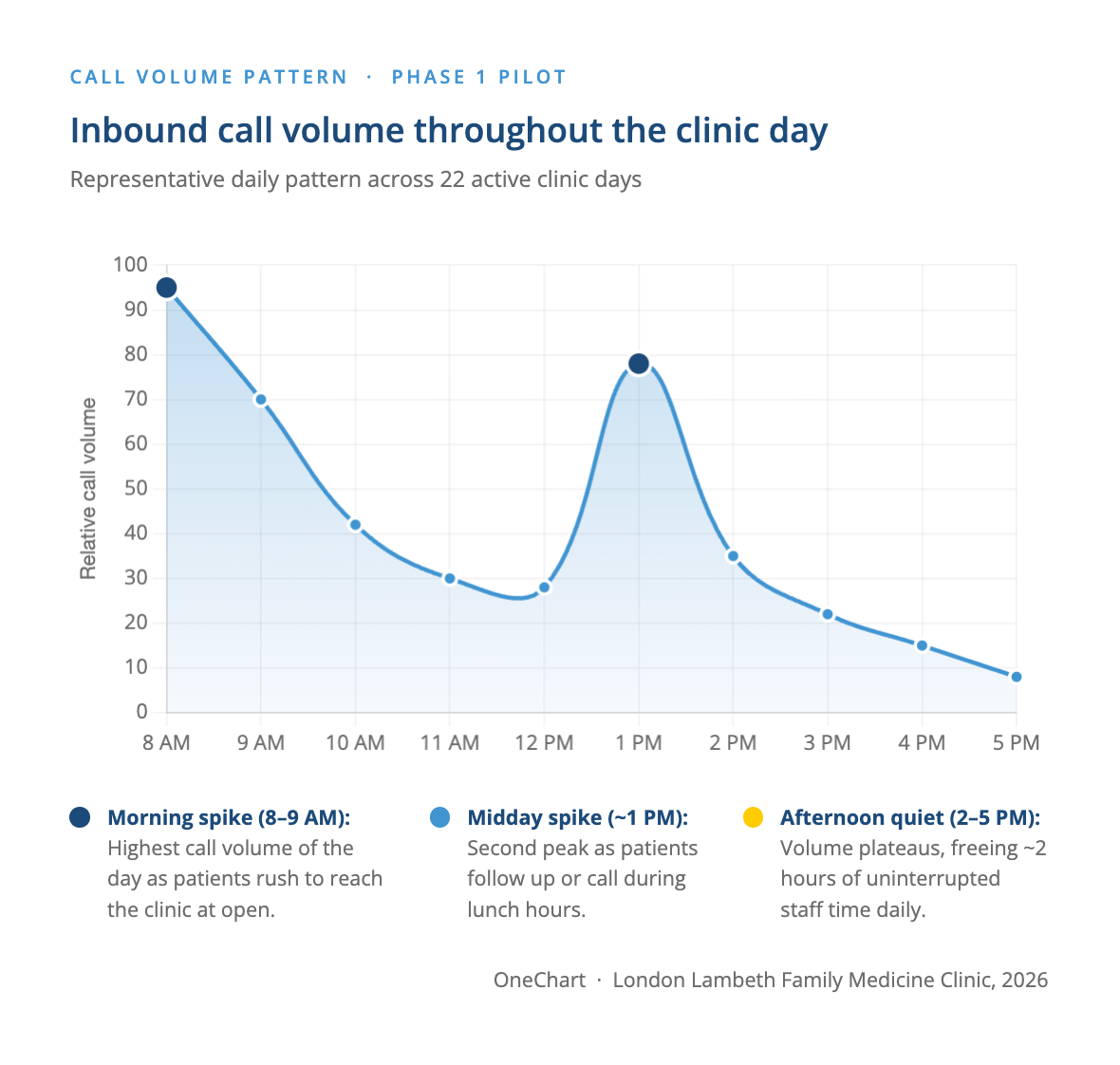
Call volume normalized by early afternoon — with the biggest spikes at 8–9 AM and again around 1 PM, the AI absorbed peak load and freed admin staff for roughly two uninterrupted hours each afternoon.
Dr. Pepe noted the speed of iteration as one of the standout strengths of the partnership. "Within the first two weeks, I think we were emailing daily or twice daily. Your team is so highly responsive to the feedback — once a change happens, it just works."
Before going live, Dr. Pepe put the agent through its paces in the most realistic test environment imaginable: his minivan, with four kids screaming in the background. "It worked with the interruptions. It worked with my kids screaming in the back of the car. It worked when I said I was having a medical emergency — the guardrails came up." That stress test was enough to convince him.
The clinic went live with the intention of shutting it off and evaluating after day one. They haven't turned it off since.
Privacy, Compliance, and Patient Trust
Patient data privacy was the most common audience question, and both Shreyas and Dr. Pepe addressed it directly.
OneChart's platform is built to support PHIPA and PIPEDA compliance, with secure encryption, data residency, and access controls as core foundations. Retention periods are configurable by the practice: where data can be removed, either on review, or at predefined windows such as a 24 hour, 7 day, or 30 day period - depending on the clinic's or an organization’s policies and preferences.
Additionally, from a workflow perspective, every interaction begins with the AI informing callers that they're speaking with an automated line, that it is not for emergencies, and that they may opt out at any time. Patients who prefer not to interact with AI can simply leave a callback number and a staff member will follow up directly.
IDENTOS's secure access exchange and Federated SSO adds a critical governance layer on top of this — ensuring that only authorized team members can log in and access the patient message dashboard, with access controls that meet the highest standards for Ontario health data. This is the same infrastructure IDENTOS has been building and refining across provincial health systems since 2014.
Interestingly, Dr. Pepe noted that some patients actually prefer leaving information with the AI, particularly for sensitive or personal matters. "They feel more comfortable just leaving their details."
The Data Gap: Who Has Real-Time Visibility?
The final poll surfaced one of the most important, and underappreciated, gaps in primary care operations today.
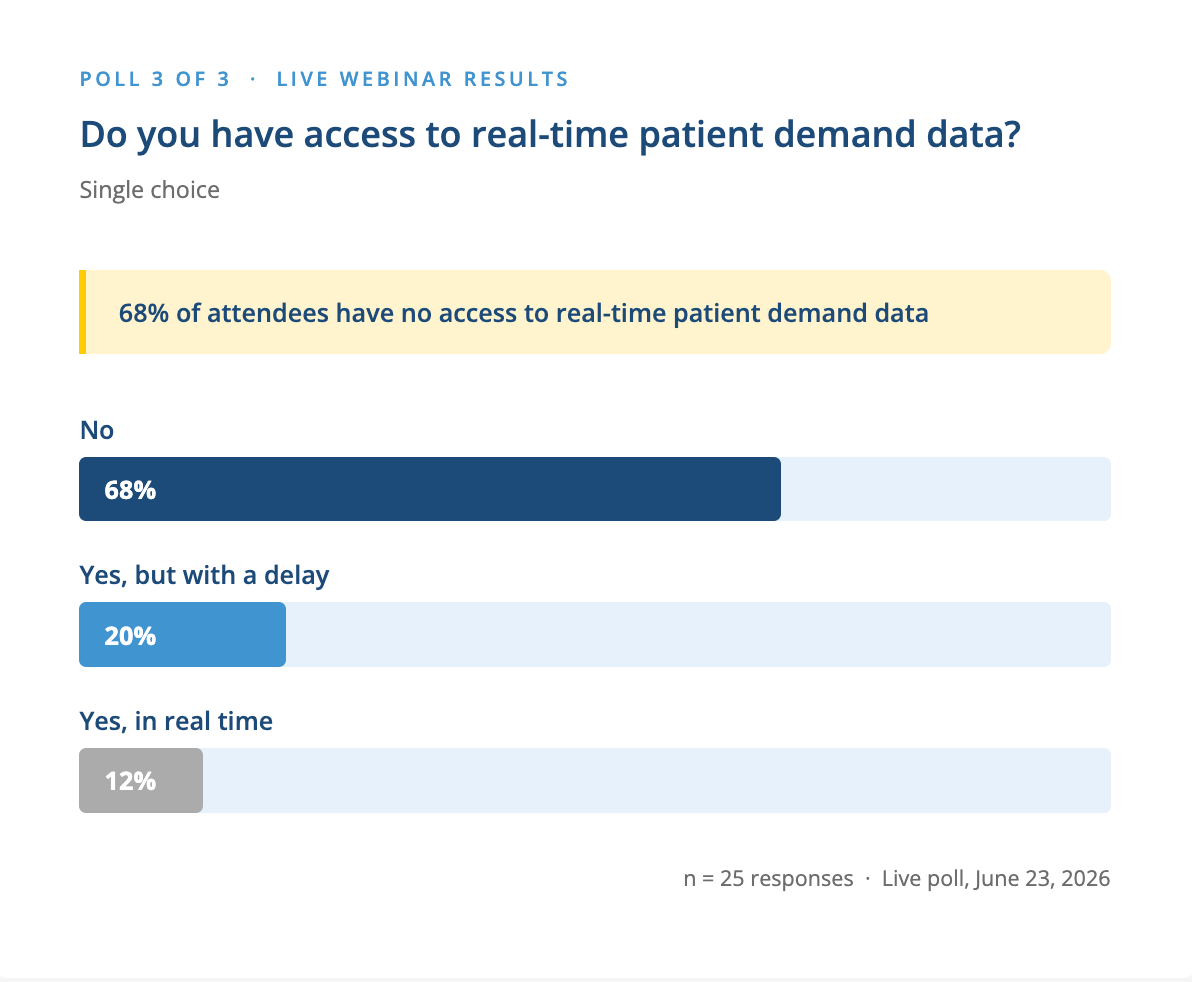
Only 12% of respondents have access to patient demand data in real time. For a system under the kind of capacity pressure Ontario primary care is facing, this is a significant blind spot. As Dr. Pepe described, the call volume and pattern data from OneChart's dashboard now directly informs how he manages after-hours capacity — in real time, as the day unfolds.
A Note on Implementation
For clinics considering this type of solution, the webinar offered a clear-eyed look at what deployment actually looks like. Dr. Pepe's team went from first conversation to live deployment in about 10 days. OneChart's phased approach — starting simple, then adding complexity — means clinics don't need to have every workflow perfectly mapped before getting started. In fact, the process of deploying often helps clarify those workflows.
"The deployment will also help you clarify your processes if you're not clear." — Dr. Dan Pepe
Because the IDENTOS access layer is already in place from day one, future expansion, toward EMR integration, multi-location analytics, or broader OHT data sharing, doesn't require rebuilding the governance foundation. It's already there.